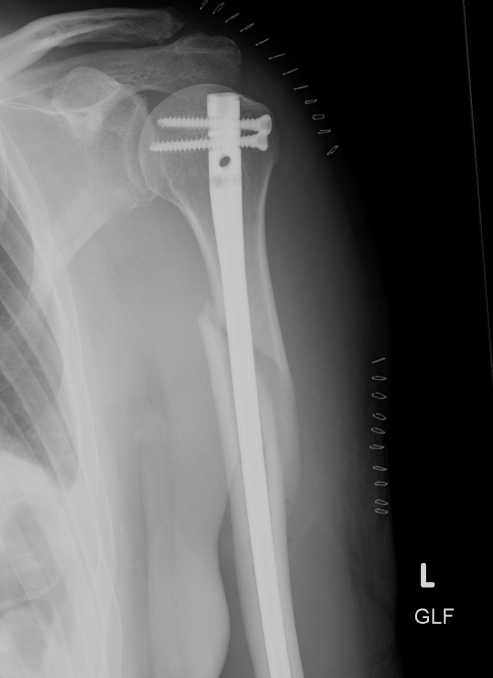
Midshaft and Proximal Third Humerus Fractures
Operative Management of Humeral Shaft Fractures
Options


Metaphyseal
Extra-articular

< 60 with good bone stock and preserved joint space
Union rates increased with anatomical reduction
Options
- closed reduction
- open reduction / if closed reduction fails
Accept
- no varus
- < 15o valgus
- < 10o AP plane
Non-union
- arrest of progression to union at fracture site
- > 6-9 /12
- no visible progressive signs of healing for at least three consecutive months
- individualise for each fracture
- when the surgeon believes the fracture has little or no chance to heal
Delayed union
- failure of fracture to unite within expected time
- still may spontaneously unite
Direct blow
- most common
Indirect
- forced knee flexion with foot fixed / maximally contracted quadriceps
1. Vertical

2. Transverse

Usually young patients
- 15 - 40
15% compound
High velocity injury
- MBA
- MVA
- pedestrian v car
- fall from height
EMST principles
- need for transfusion not uncommon
Resuscitation
EMST
Neurovascular assessment
Investigations - exclude Pipkin, NOF
Emergent reduction / skeletal stabilisation
Assess stability
Re-evaluate sciatic nerve
Indications
- displaced acetabular fracture

Most common long bone fracture
Young patients / sports
Elderly / simple falls
MVA - often compound
Grade 0
- nil ST injury
Grade 1
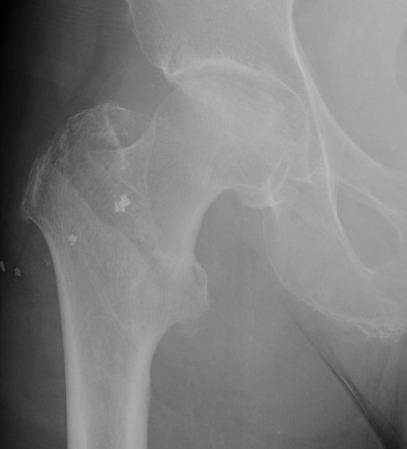
Fracture which extends between the trochanters of the proximal femur
- lower limit is inferior border of lesser tuberosity
Extra capsular / well vascularized
The key to stability is the posteromedial cortex
Non-anatomical bony block
- transfer of coracoid process through subscapularis
- dynamic anteroinferior musculotendinous sling
- provides subscapularis tenodesis
- preventing lower portion from displacing proximally as arm abducted
- when shoulder in vulnerable position abduction and ER