
Epidemiology
Most common form of shoulder instability
Most common in young males
- US database of 9000 shoulder dislocations
- 72% male
- 47% between 15 and 29
- 48% occurred during sports
Etiology
Fall on outstretched arm
Indirect external rotation and abduction moment on arm
Examination
Very painful & tender shoulder
Arm held across abdomen
Hollow under acromion and fullness in anterior shoulder
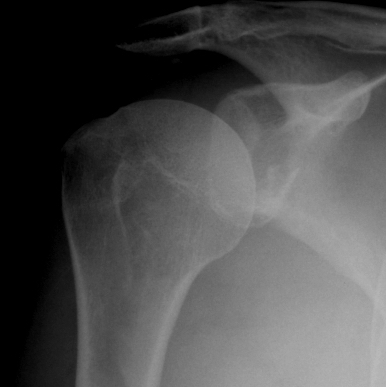
Xray
True AP

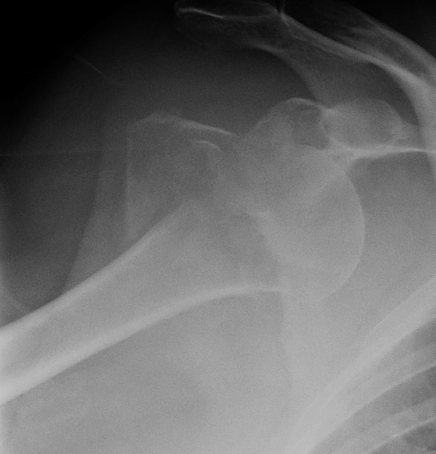

Scapular Lateral

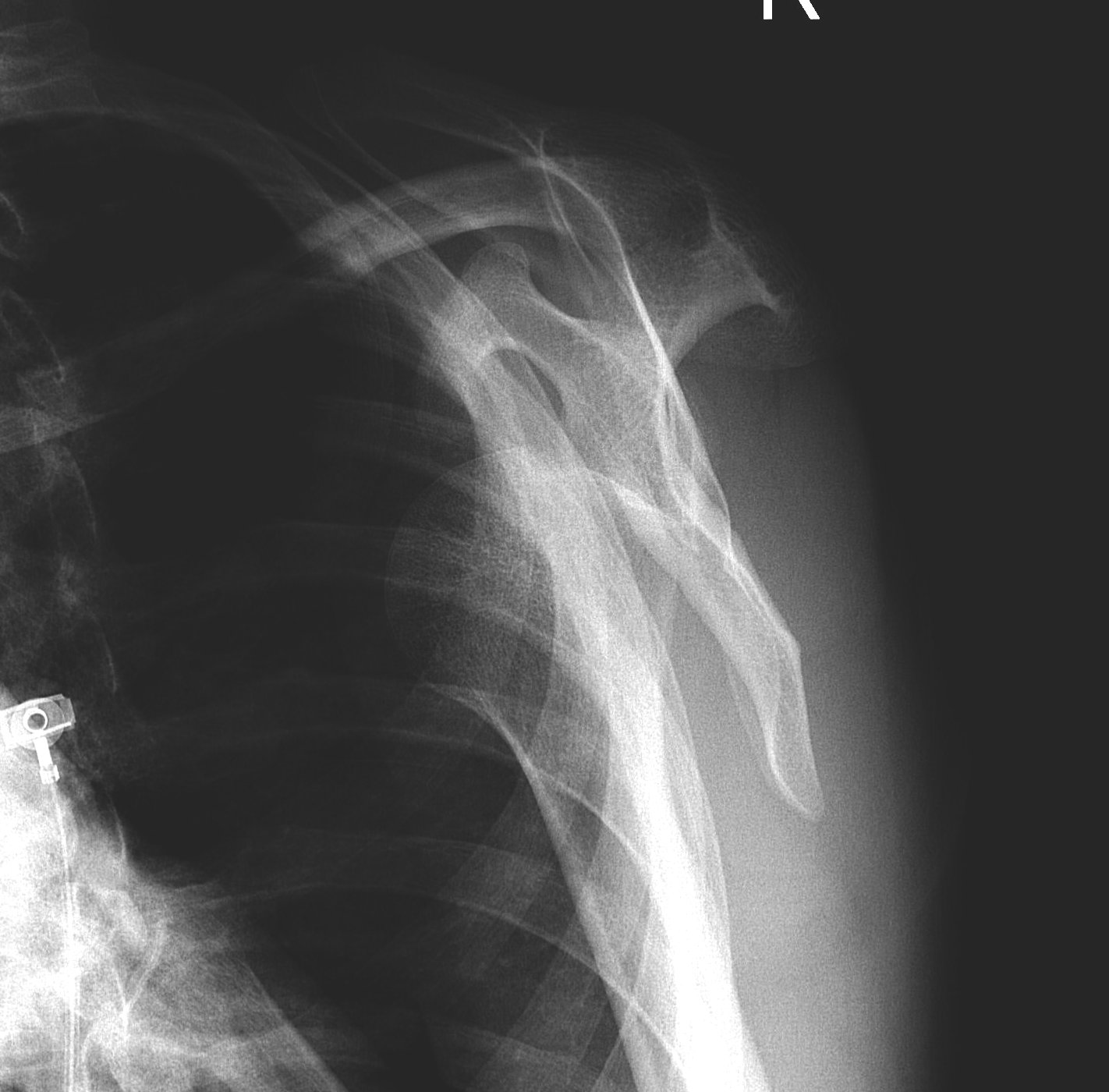
Axillary Lateral



Garth (aim beam caudally)

Management
Reduction techniques
| Stimpson |
Harvard Traction /Countertraction method |
Kocher | Hippocrates |
|---|---|---|---|
|
Patient prone Arm hanging over side of bed Weight applied to wrist |
Patient supine Traction with abduction Countertraction via sheet around axilla |
Externally rotate and maximally abduct arm Relocate via adduction Nil IR til located to avoid humeral fracture |
Foot in arm pit Apply longitudinal traction |
 |
+/- conscious sedation | +/- conscious sedation | +/- conscious sedation |
Rehabilitation
Sling versus external rotation brace
- RCT ER brace v sling 198 patients 3 weeks duration
- 26% recurrence external rotator brace
- 42% recurrence in normal sling
- RCT ER brace v sling 188 patients 3 weeks duration
- 31% recurrence external rotator brace
- 25% recurrence in normal sling
Duration of immobilization
Prognosis
- national database 1000 patients with first time shoulder dislocation
- redislocation rates at 5 years
- age 10-19: 49%
- age 20 - 29: 28%
- age 30 - 59: 14%
- age >60: 17%
Surgery for first time dislocation
- systematic review operative v non operative for first time dislocation
- arthroscopic bankart repairs
- 10 prospective studies with 569 patients
- redislocation: surgery 10% v 67%
- further surgery: 7% v 47%
- return to sports: 93% v 81%
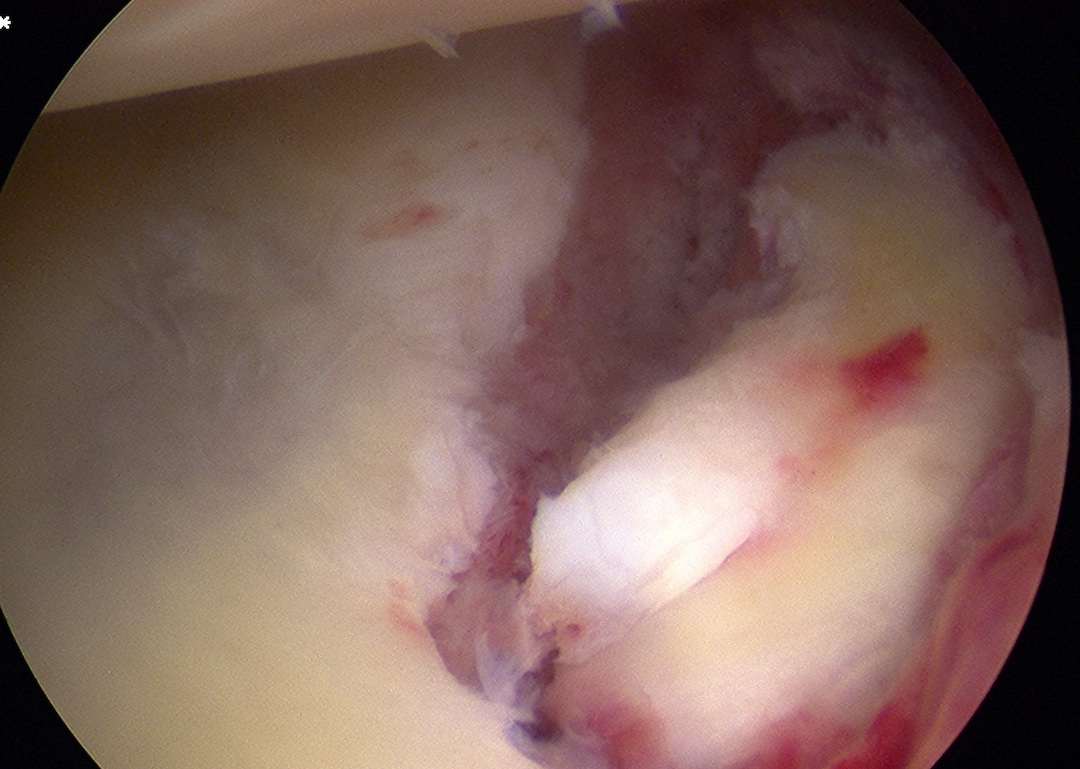
Associated injuries
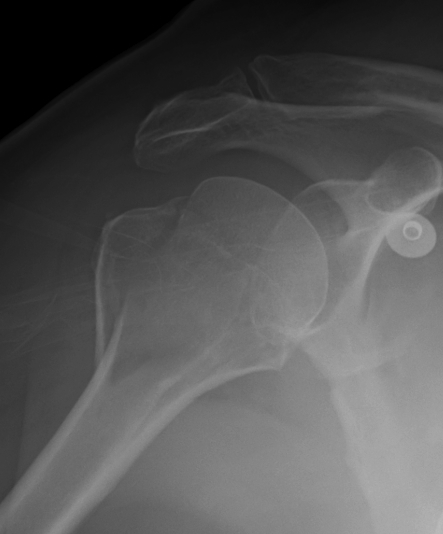
Bony bankart / glenoid rim fractures

Indications for surgery
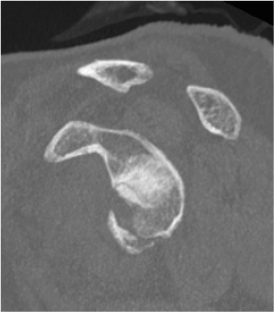
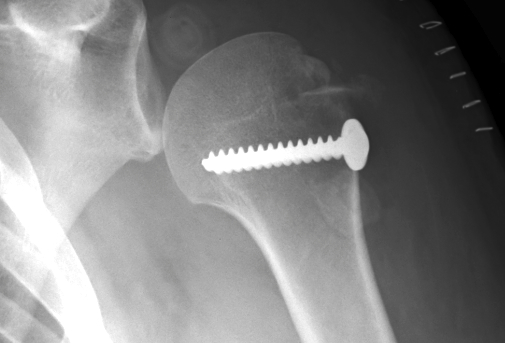
Glenoid fossa fractures
- 25 - 30%, displaced
- open v arthroscopic screw fixation
www.boneschool.com/glenoid-fractures
Acute bony bankart / glenoid rim fractures
- ? acute repair to reduce instabilty
- ? avoid Latarjet procedure later
Results
- systematic review of arthroscopic bony bankart repair
- 21 studies with 769 patients
- recurrent instability 12%
- return to sport 91%
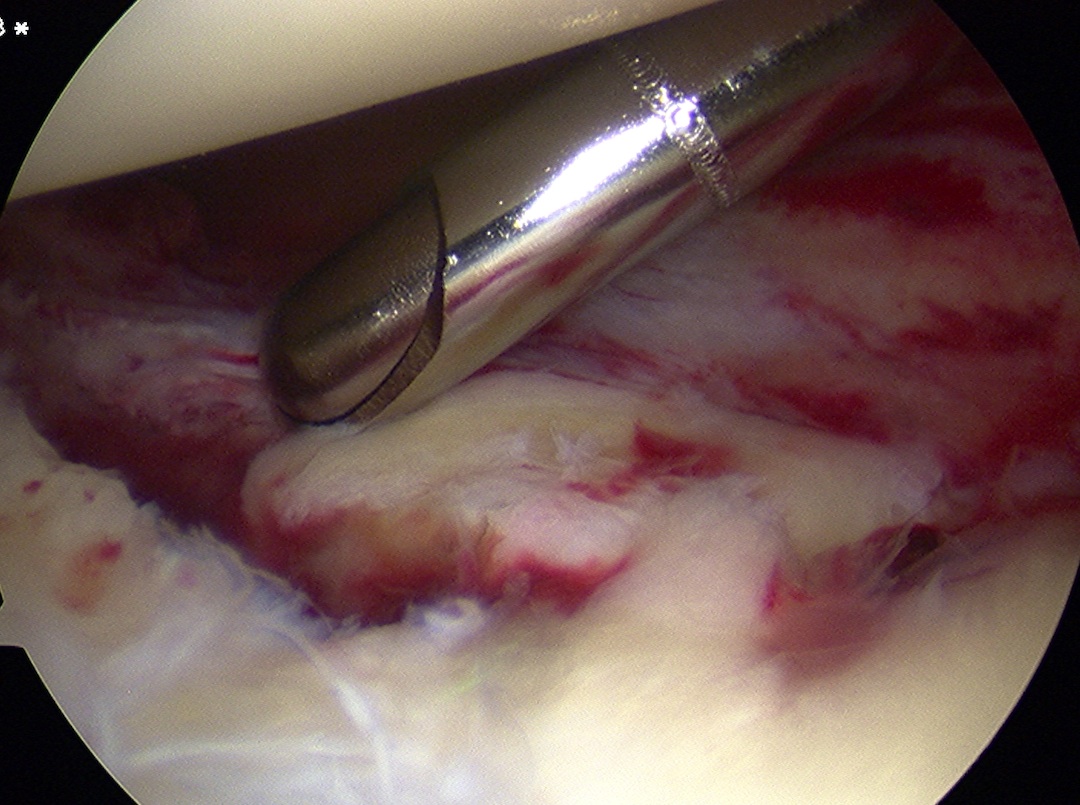
Technique

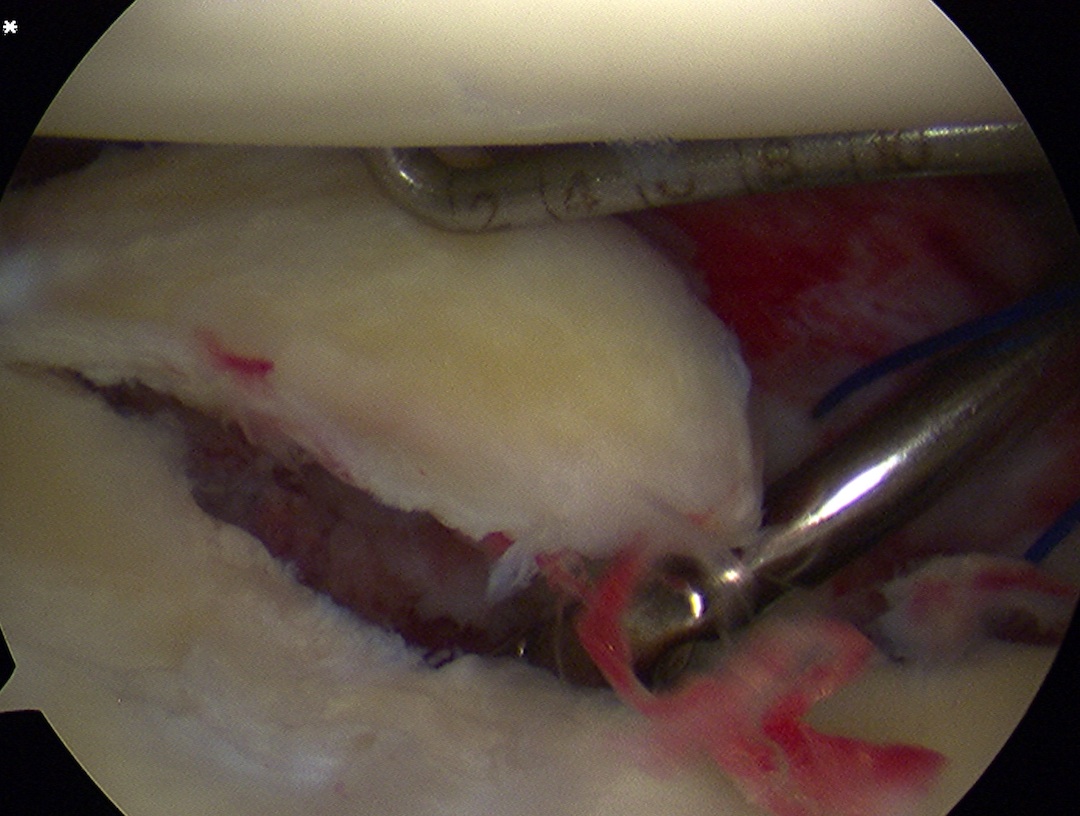

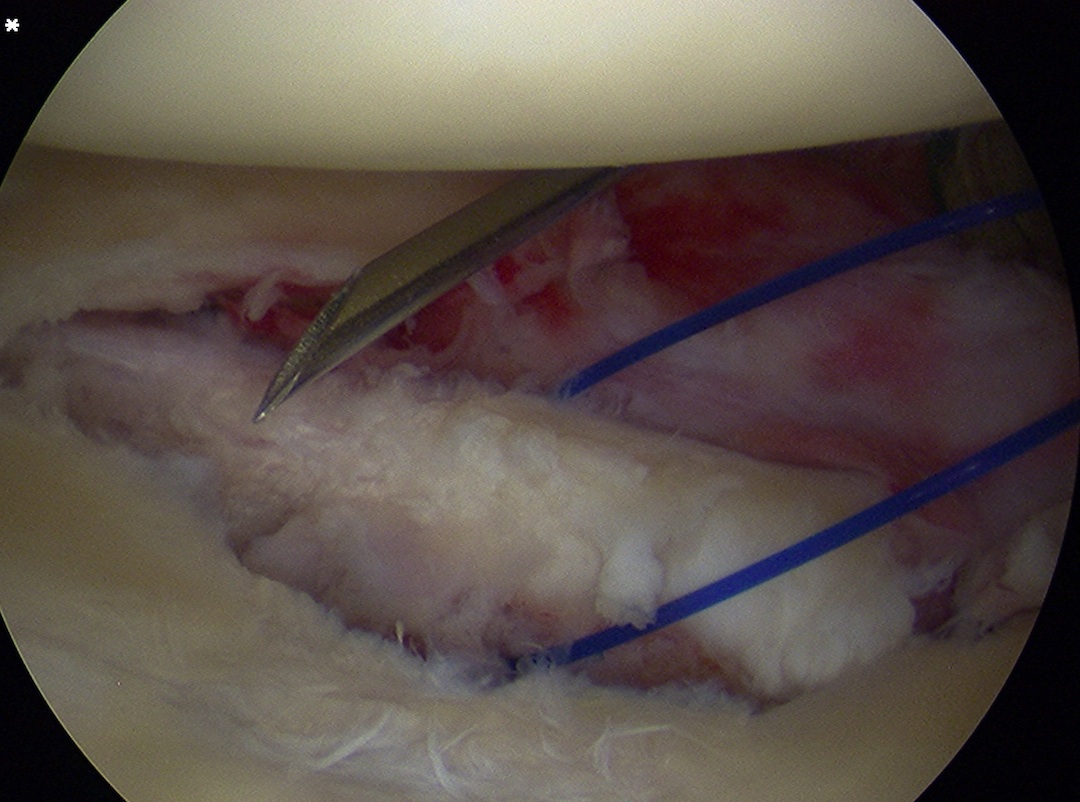

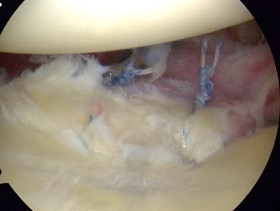
Arthroscopic suture anchor fixation bony bankart
Vumedi arthroscopic anchor fixation glenoid fracture video
Arthroscopy techniques anterior glenoid rim arthroscopic anchor fixation PDF
Greater tuberosity fractures
Indications
- > 5 mm displacement
Management
- ORIF with plate
- screw + suture repair
- screw alone in young patient
www.boneschool.com/greater-tuberosity-fractures
Rotator Cuff Tear


Infraspinatus and supraspinatus wasting after shoulder dislocation in 50 year old
More common in older patients with shoulder dislocation
- 66 patients > 50 with shoulder dislocation
- 60% rotator cuff tear on MRI
Nerve injury
Axillary nerve palsy - most common

- 240 cases of anterior shoulder dislocation
- 16% axillary nerve injury
- half isolated injuries
- patients with isolated axillary nerve injury after shoulder dislocation
- average age 64
- 22/28 axillary nerve injuries recovered
Musculocutaneous Injury


Wasting of the left biceps after shoulder dislocation in setting of anterior shoulder dislocation
Brachial plexus injury
- 61 patients with brachial plexus injury after shoulder dislocation
- infra-clavicular cord injuries
- average age 64
- 11/11 lateral cord injuries recovered spontaneously
- 20/24 posterior cord injuries recovered spontaneously
- recovery of medial cord / intrinsic hand muscles worst (14/27 poor recovery)