
Definition
Frozen shoulder
Idiopathic inflammatory condition characterised by progressive shoulder pain & stiffness
- patients develop contracture of capsuloligamentous structures
- spontaneously resolves
Epidemiology
3% incidence in population
20% in diabetics
40 - 60 years
Women:Male 2:1
Bilateral in 10 - 40%
Etiology
| Primary | Secondary |
|---|---|
| Unknown ? Autoimmune |
Following insult |
|
Associations - Diabetes - Thyroid disease - Stroke / Myocardial infarct / heart surgery - Depuytrens |
Post shoulder surgery Post shoulder fracture / dislocation Prolonged shoulder immobilization |
Classification Neviaser
Each lasts 4-8 months
Inflammation followed by fibrosis
| Freezing | Frozen | Thawing |
|---|---|---|
| Painful |
Decreasing pain Increasing stiffness |
Spontaneous resolution Stiffness begins to improve |
|
Capillary proliferation / Synovial hypertrophy Develop capsular adhesions |
Maturation Capsular contraction |
Typically begins 12 months from onset |
Pathology
Primary
- contracture of capsuloligamentous structures
- initial synovitis of unknown cause
- capsulitis
- contractures
- a dense matrix of type 1 and II collagen laid down by fibroblasts and myofibroblasts
Secondary
- much less synovial inflammation
Natural History
Traditionally thought to be benign & self-limiting
- 4 year follow up of 220 primary frozen shoulder
- 59% normal or near normal
- 41% ongoing symptoms, with majority having mild pain
- 2.5% had severe ongoing pain and functional loss
History
Initial insidious onset of pain with gradual reduction in ROM
Pain resolves over 6 months but stiffness remains
Examination
Markedly decreased ROM both active and passive
Limited active and passive external rotation
Differential diagnosis of reduced passive external rotation
- Frozen shoulder (normal xray)
- OA (abnormal xray)
- Unreduced posterior dislocation (abnormal xray)
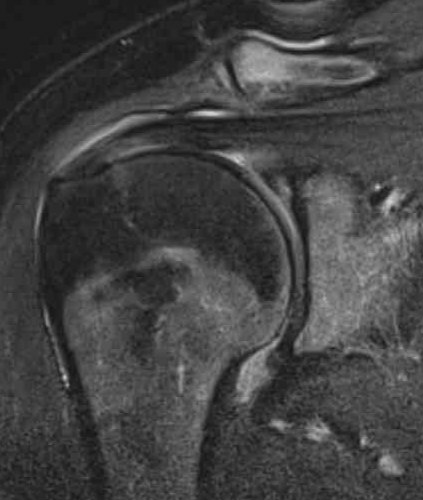
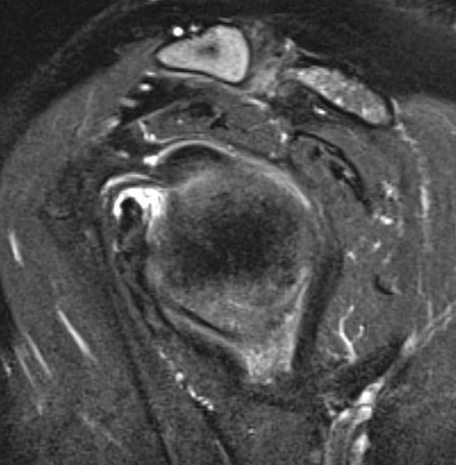
MRI
Thickened capsule and synovitis of axillary capsular recess

Management
Options
Physiotherapy
ECSW
Intra-articular injections
Manipulation under anesthesia (MUA)
Hydodilatation
Arthroscopic capsular release
Physio+cortisone v MUA v arthroscopic capsular release
UK Frost Study Group Lancet 2020
- RCT of 500 patients with frozen shoulder with 1 year follow up
- 12 weeks physiotherapy + cortisone injection v MUA v arthroscopic capsular release
- no treatment superior to the other
- MUA most cost effect
- capsular release highest adverse events
Physiotherapy
Nakandala et al J Back Musculoskeletal Rehab 2021
- systematic review of physiotherapy modalities for adhesive capsulitis
- some evidence for reduction in pain and improvement in ROM
Extracorporeal shockwave therapy (ECSW)
- systematic review of ECSW in adhesive capsulitis
- improved outcomes and short term pain relief with ECSW
Intra-articular injections
Indication
- freezing stage
- aim to reduce pain
Cortisone
- intra-articular cortisone v control
- systematic review of 8 RCTs and 400 patients
- cortisone injections improved range of motion / outcome scores / pain scores
- up to 6 months
Hyaluronic acid (HA)
Mao et al J Orthop Surg Res 2022
- intra-articular HA v control
- systematic review of 7 RCTs and 500 patients
- no real difference in pain scores or ROM
PRP
Zhang et al BMC Musculoskeletal 2024
- intra-articular HA v control
- systematic review of 14 RCTs and 1000 patients
- PRP improved pain, ROM and outcome scores compared to controls
- superior to cortisone
Manipulation under anesthesia
| Timing | Contra-indications | Complications |
|---|---|---|
|
After 6 months |
Osteopenia | Fractures / dislocations |
| Frozen or thawing stage | Previous surgery | Rotator cuff tears |
Technique (Neviaser)
GA / interscalene block
- abduction first: gentle, release scarred axillary fold
- rotation: gentle, in abduction, highest risk of spiral fracture
- +/- cortisone
- +/- hydrodilatation
Results
Salomon et al Int J Environ 2022
- systematic review of MUA and other treatments
- limited evidence that MUA superior to physiotherapy / home exercise at 1 year
Hydrodilatation
Concept - disrupt thickened contracted tissue with high water pressure
Technique
Ultrasound guided technique PDF
Ultrasound guided
- injection local anesthetic + cortisone
- inject 50 mls of normal saline
Results
Lin et al Arch Phys Med Rehab 2018
- systematic review of hydrodilatation v steroids
- no difference in functional improvement or pain
- improved external rotation with hydrodilatation
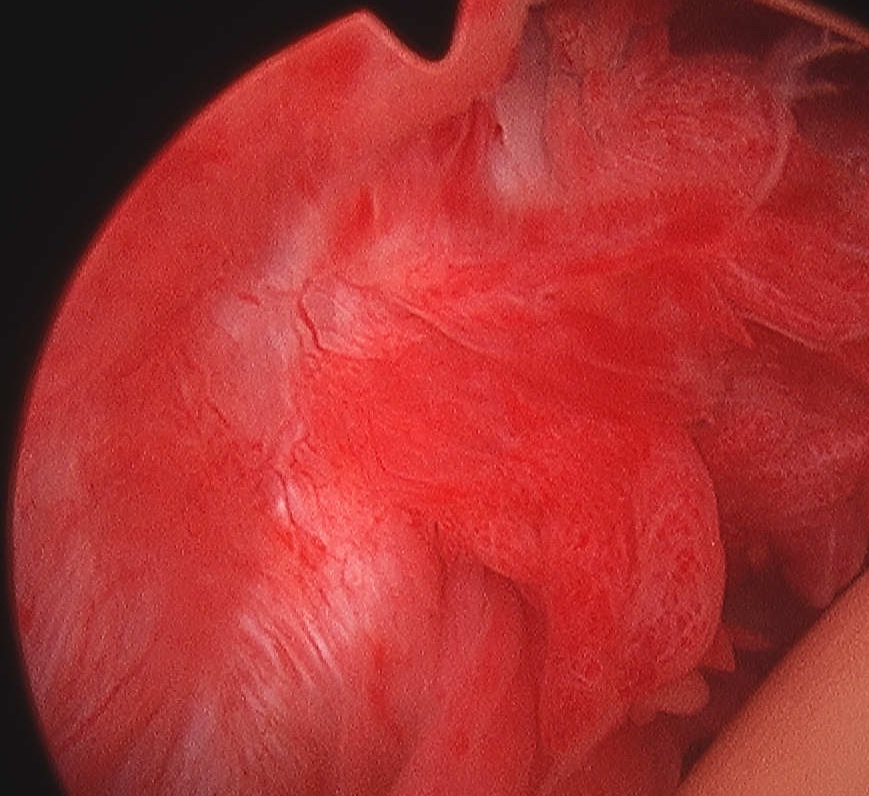
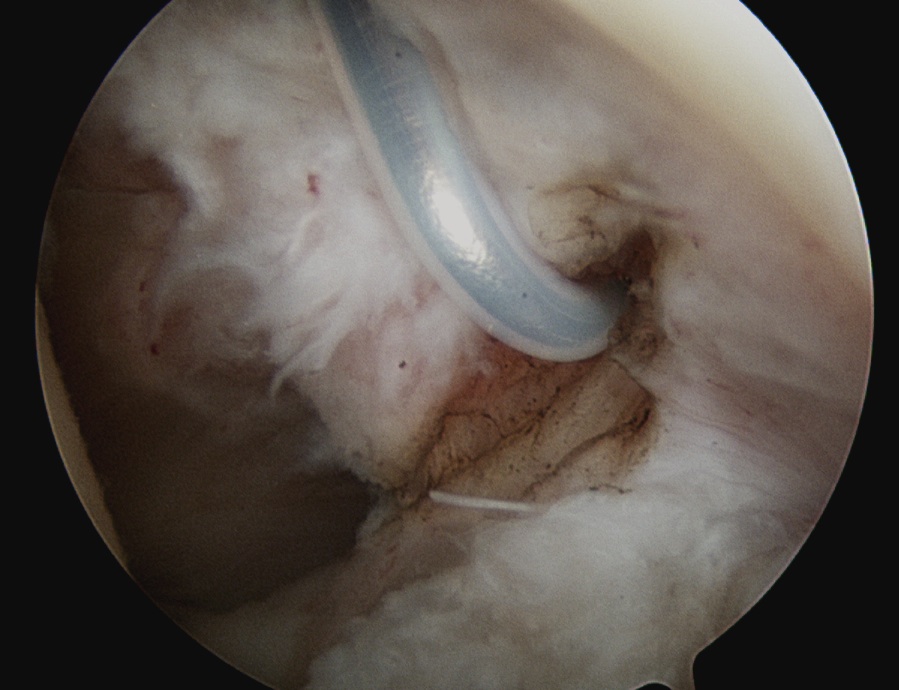
Arthroscopic capsular release
Technique
Vumedi frozen shoulder arthroscopic capsular release video
Arthroscopy techniques frozen shoulder 360 degree release PDF
Release rotator interval - remove all tissue in between biceps and SSC
Mobilze subscapularis front and back from scar tissue
Release anterior IGHL from 3 to 5 o'clock, leaving labrum intact
Release posterior IGHL from 9 to 11 o'clock, leaving labrum intact
+/- release inferior capsule, beware injury to axillary nerve
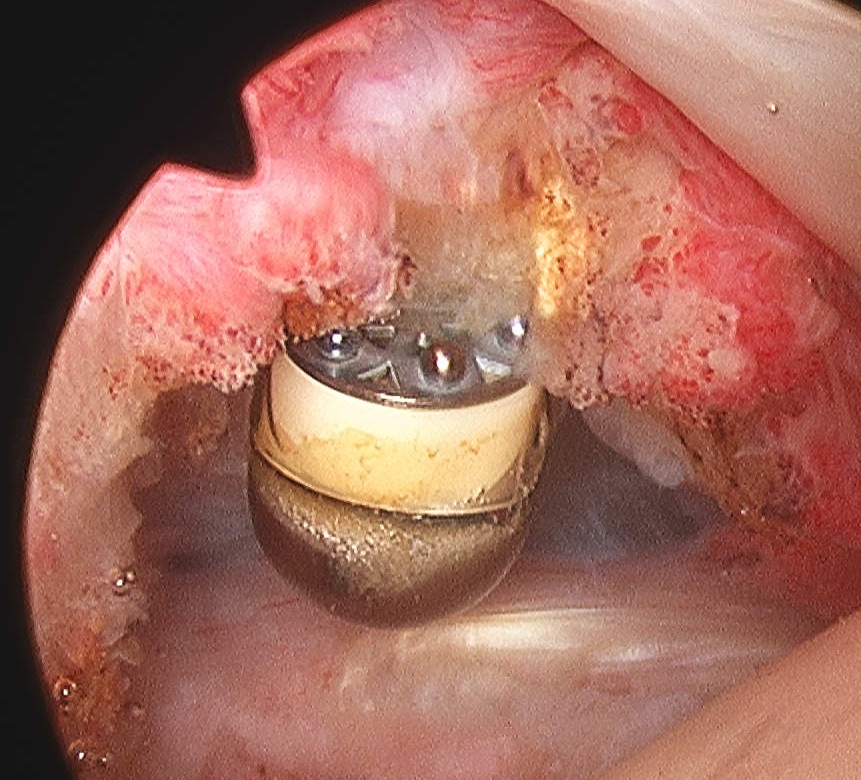
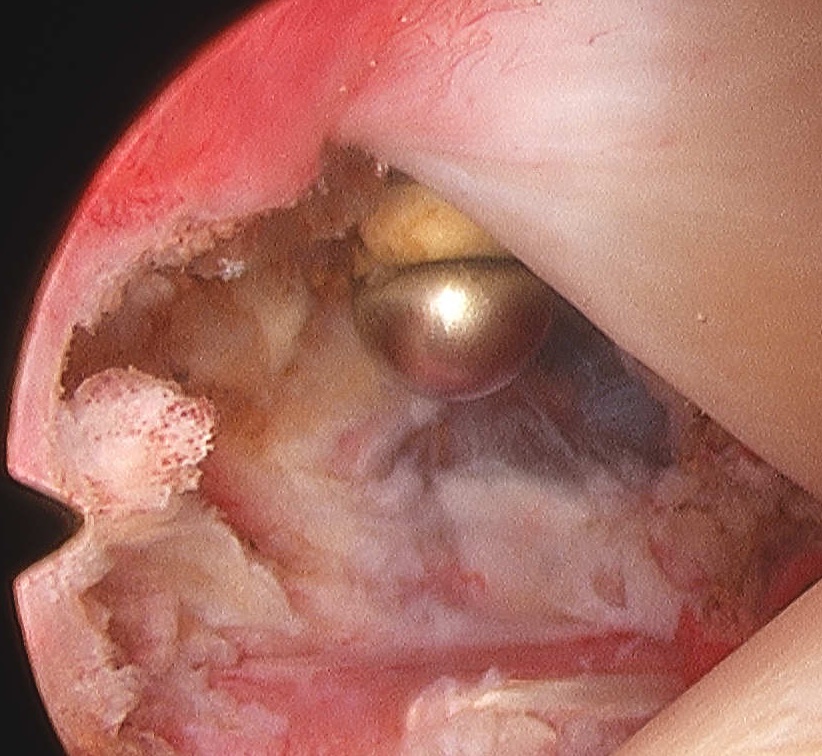
Rotator interval release

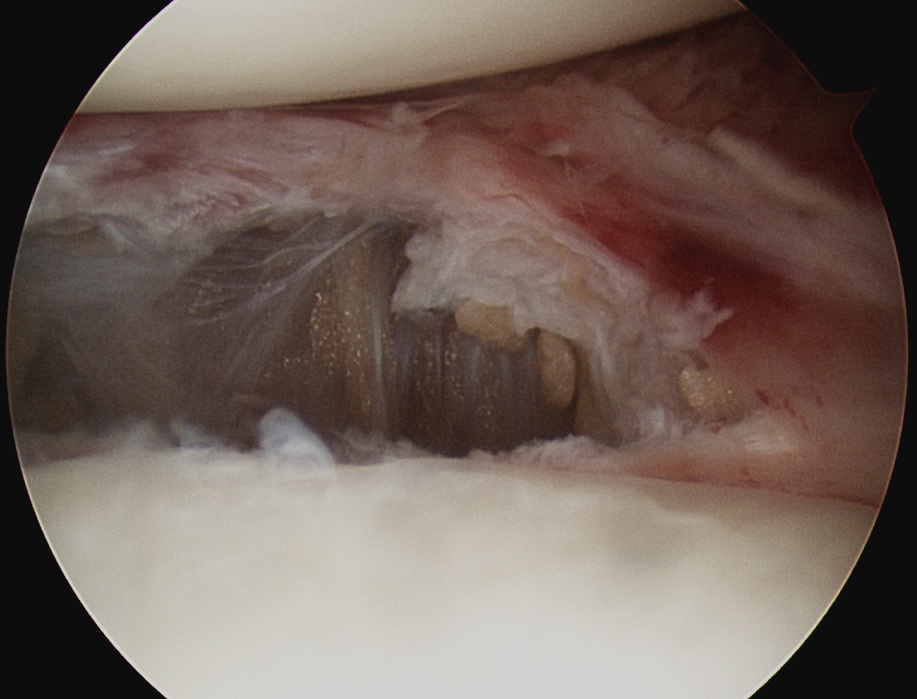
Release anterior IGHL
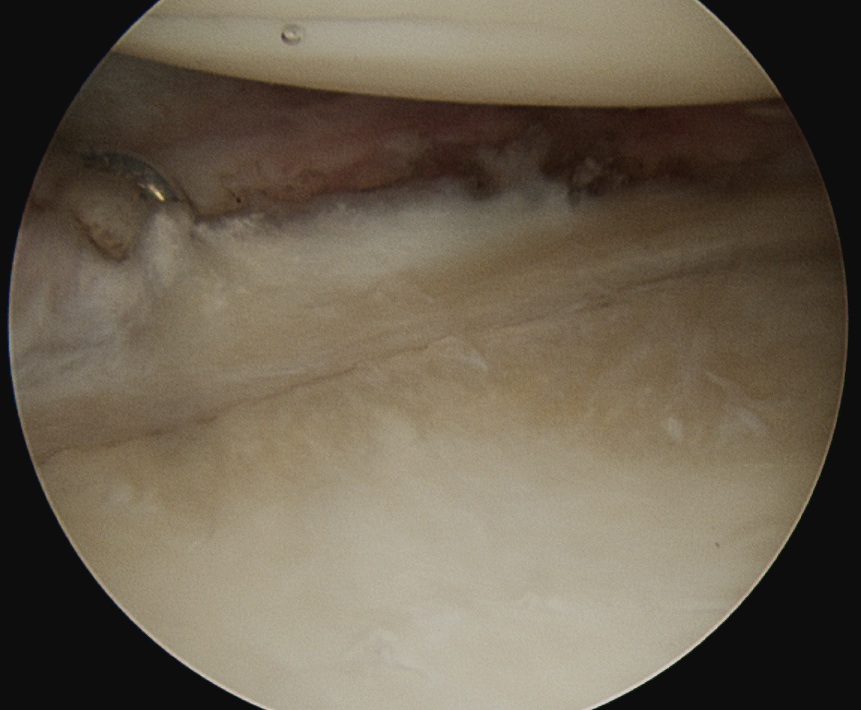
Release posterior IGHL
Results
- RCT of 74 patients with frozen shoulder
- anterior release versus anterior/posterior release
- no difference in ROM at 6 months
- better ROM at 3 months in anterior / posterior release