

Epidemiology
Second most common dislocation after shoulder
Most common 10 - 19 year age group
Mechanism
FOOSH
Classification
| Direction of dislocation | Degree of dislocation | Simple / Complex |
|---|---|---|
| Posterior / posterolateral | Complete | Simple - no fractures |
| Final position of ulna relative to humerus | Subluxed / perched 10% | Complex - fractures |


Perched elbow dislocation / subluxation
Bony Anatomy
| Ulnohumeral Joint | Radiocapitellar Joint | Distal Humerus |
|---|---|---|
|
Trochlea and ulna highly conformed - trochlea covered by cartilage in arc 300o - trochlea separated from the capitellum by groove - trochlea 6o valgus which creates carrying angle
|
Concave radial head - articulates with capitellum - posteromedial 2/3 articulates with sigmoid notch ulna - anterolateral 1/3 has no cartilage / safe zone |
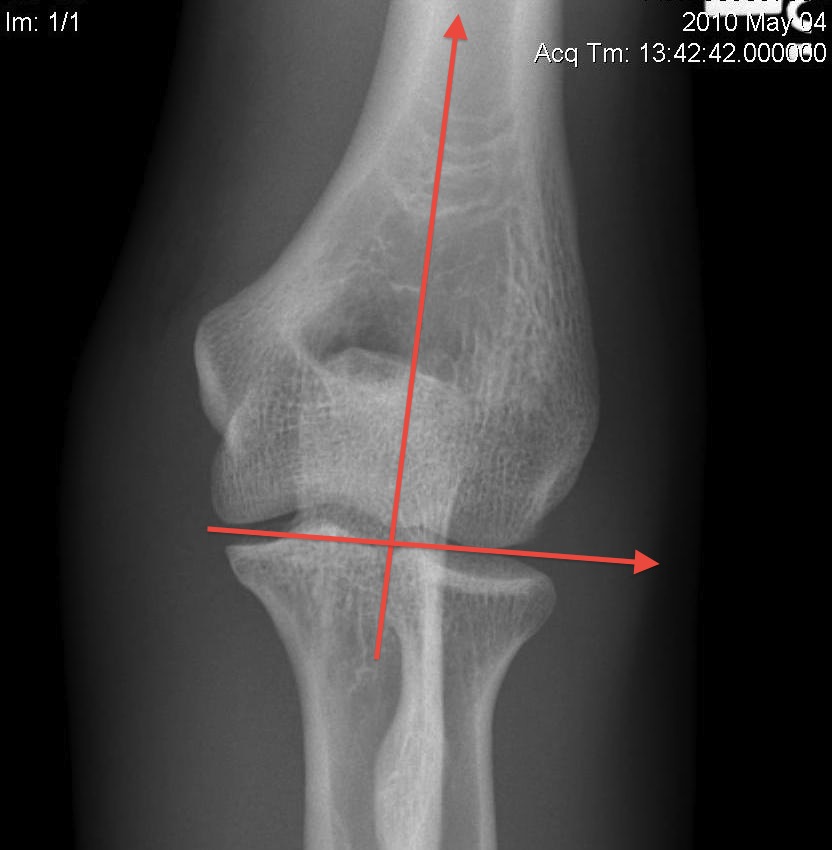
Tilted anteriorly 30o in lateral plane - 5o internally in transverse plane - 6o of valgus in front plane |
|
Radial head important secondary stabiliser, especially when MCL deficient
|
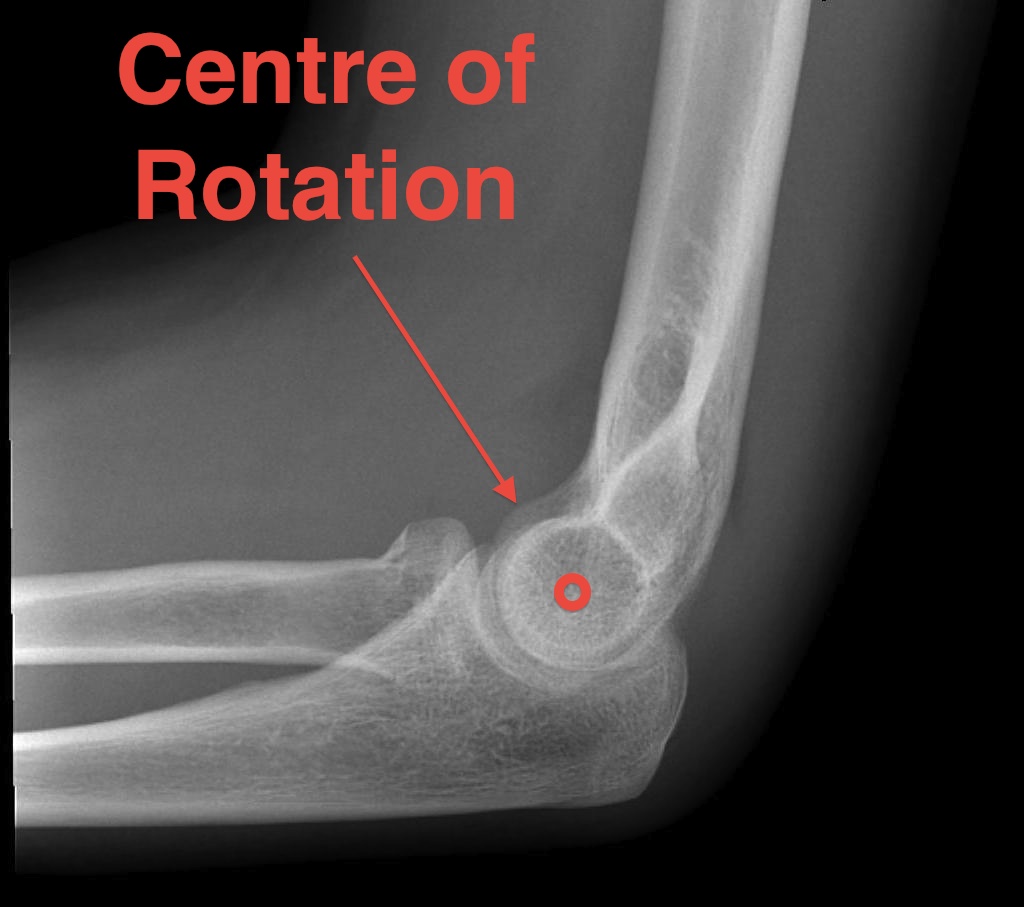
Centre of rotation - trochlea - centre of rotation anterior to humeral shaft |

Ligaments
| Lateral collateral ligament | Medial collateral ligament |
|---|---|
| Provides varus stability |
Provide valgus stability in flexion |
| Four components | Three components |
|
1. Lateral Ulna Collateral Ligament - most important - lateral epicondyle to supinator crest
2. Radial Collateral Ligament - lateral epicondyle to annular ligament
3. Accessory Collateral Ligament - lateral epicondyle to annular ligament and supinator crest
4. Annular Ligament - anterior and posterior sigmoid notch
|
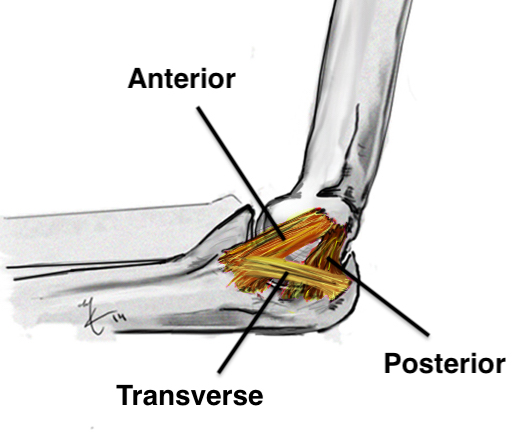
1. Anterior band - most important - medial epicondyle to sublime tubercle
2. Posterior band - medial epicondyle to olecranon
3. Transverse band - olecranon to sublime tubercle - groove for ulna nerve
|
 |
 |
Elbow stabilizers
| Primary Static | Secondary Static | Dynamic Stabilisers |
|---|---|---|
|
Ulnohumeral joint / coranoid process - 50% of stability
|
Radiocapitellar joint Radial head |
Anconeus |
|
Anterior bundle of MCL - valgus stability
|
Anterior capsule | Common flexor / common extensor muscles |
|
LCL - varus stability - posterolateral stability radial head
|
Biceps / brachialis / triceps |
Elbow dislocation patterns of injury / Horii circle of disruption
Begins on the lateral side
- progresses to the medial side in three stages
- anterior band of MCL is the last torn
| Stage 1 | Stage 2 | Stage 3 |
|---|---|---|
| Tear LCL | Tearing of anterior capsule |
Stage 3A - posterior band MCL torn - anterior band MCL intact - posterior dislocation
After reduction elbow stable with hand pronated
|
|
Posterolateral rotatory subluxation / instability
|
Incomplete posterolateral dislocation Coranoid perches on trochlea |
Stage 3B - anterior band of MCL also torn - elbow needs to be flexed to > 30 - 40o to be stable
|
|
Stage 3C - MCL torn and CFO /CEO torn - elbow needs to be flexed > 90o to be stable
|
Simple versus Complex elbow dislocation
Simple
- pure ligamentous injury
- no fractures
Complex
- radial head fracture
- coronoid process fracture
- Terrible Triad (MCL + coronoid + coronoid fracture + radial head fracture )
- olecranon fracture +/- radial head +/- coronoid
- capitellar fractures
Acute Elbow Dislocation
Management
1. Reduction under conscious sedation
Traction / countertraction
- use thumbs to correct lateral displacement / push olecranon medially
- flexion to 90o
Youtube elbow dislocation reduction technique video
Youtube elbow dislocation reduction technique video 2
Youtube elbow dislocation reduction technique video 3
2. Assess stability post reduction
Elbow stable - extend to within 30 - 40o without redislocation
Elbow unstable - pronate forearm and see if can extend to within 30 - 40o (MCL intact)
Elbow unstable in pronation - surgery
3. Confirm concentric reduction on xray
Stable Simple Elbow Dislocation


Definition
Elbow fracture with no fractures
Stable in full extension
Results
Operative versus nonoperative
- RCT of 30 patients with simple elbow dislocation
- surgery versus cast 90° for 2 weeks
- no difference in outcome
- increased loss of extension in operative group
Immobilization
Iordens et al Br J Sports Med 2017
- RCT of 100 patients with simple elbow dislocation
- early mobilization versus 3 weeks cast
- no redislocations
- better early recover with early mobilization
- no difference at one year
- RCT of 50 patients with simple elbow dislocation
- early mobilization versus 3 weeks cast
- increased stiffness / extension loss in cast group (19% versus 4%)
Outcomes
- 110 simple elbow dislocations at mean 7 years
- 56% reported residual stiffness
- 8% reported subjective instability
- 62% reported residual pain
Unstable simple elbow dislocation
Definition
Elbow unstable after reduction
- redislocates with extension to 30 - 40o: LCL +/- common extensor origin tear
- not stable in pronation: MCL / UCL tear
Not concentrically reduced on xrays
Management
1. Repair LCL + common extensor origin
Kocher approach
- lateral collateral ligament is usually avulsed from lateral condyle
- centre of rotation is center of capitellum
- place suture anchor and repair LCL +/- common extensor origin
- assess stability
AO Surgery Kocher & Kaplan reference
2. Elbow still unstable / repair +/- reconstruct MCL / UCL
Medial approach
- FCU split / Hotchkiss over the top approach
- identify and protect ulna nerve
- usually avulsed from medial epicondyle
- suture anchor repair +/- common pronator flexor origin
- mid-substance tears - reconstruct with Palmaris
Results
- 118 simple elbow dislocations
- 49 group 1 / mild instability - good results
- 28 group 3 / severe instability - good results with ligament repair
- 41 group 3 / moderate instability - improved outcomes and lower revision rate with ligament repair
Heo et al Clin Orthop Surg 2021
- 21 cases of unstable simple elbow dislocation
- LCL complex +/ CEO repair sufficient for stability in 81% (17/21) cases
- 19% (4/21) required additional MCL repair
- LCL repair only - 100% good or excellent results
- LCL + MCL repair - 50% good or excellent results